
Safeguarding Unborn Babies – Pre-Birth Guidance
Contents
- Aim of guidance
- Introduction
- Identification of need and Risk During Pregnancy
- Female Genital Mutilation (FGM) and Unborn Babies
- Working with Fathers
- Referrals to Children’s Social Care
- Consent
- Pre-Birth Assessments
- References
Aim of this Guidance
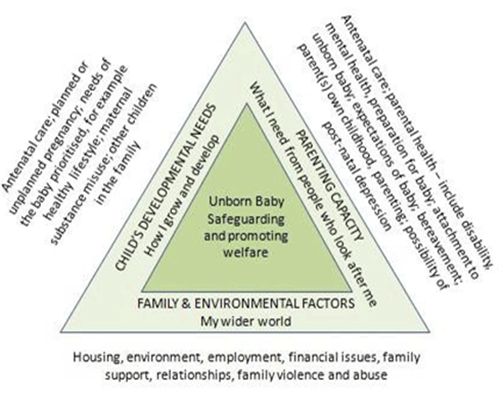
This guidance has been developed in conjunction with City of York and North Yorkshire partner agencies and seeks to assist professionals when considering safeguarding concerns relating to unborn children. It is designed to help all professionals to carefully consider a range of themes and to identify issues that have potential for having a significant negative impact on the safety and wellbeing of unborn babies. Importantly, the guidance aims to support practitioners when undertaking an assessment of risk and need.
Introduction
The 2022 analysis of serious case reviews (DfE, 2022) found that, as with previous national analyses, the largest proportion of incidents related to the youngest children, with 37% aged under 1. Of these, 47% were under 3 months of age, 29% were aged 3 to 5 months, 16% were aged 6 to 8 months, and the remaining 8% were between 9 months and 1 year at the time of the incident. This has been a pattern in Child Protection since records began to be kept and seems to relate to 3 factors – physical vulnerability of the infant; their invisibility in the wider community and inability to speak for themselves; and the physical and psychological strain their presence places upon their caregivers. It is critical, therefore, that Local Safeguarding Children’s Partnerships (LSCPs) have robust procedures in place, both to identify the unborn children most at risk and then to effectively manage their welfare and safety at the earliest opportunity.
The nature of safeguarding work dictates that the most successful preventative action can be taken if vulnerable children are identified as early as possible – this includes identifying such children during pregnancy. This early warning system can only operate in a meaningful way if there is an agreed interagency commitment to the importance of this area of safeguarding, and that all professionals work together to assess and manage the response to this high-risk group.
Identification of Need and Risk During Pregnancy
Parents and family who may require additional support:
The identification of need and risk in pregnancy may be due to parents and close family members requiring additional support; this may include the mother, biological father, and mother’s partner (if different to the biological father).
- Parents with Learning Disabilities who may need help to manage caring for a young child –
‘A learning disability is a lifelong condition; it is not an illness and cannot be cured.
The term learning disability is used in relation to individuals who have the following characteristics:
- ‘Impaired intelligence’ (Reduced ability to understand new or complex information, to learn new skills)
- ‘Impaired social functioning’ (Reduced ability to cope independently)
A condition which started before adulthood and has a lasting effect’. A learning disability affects the way a person understands information and how they communicate. This means they may have difficulty understanding new or complex information, learning new skills, or coping independently. A learning disability can be mild, moderate, or severe and if someone with a learning disability had an IQ test this would score under 70.
Having a learning disability and learning difficulties should not be confused. A learning difficulty is a difficulty in learning which includes dyslexia, dyspraxia/developmental co-ordination disorder (affecting physical co-ordination) and attention deficit hyperactivity disorder (ADHD). A person with a learning disability may also have one or more learning difficulties. It is also important to recognise that someone can be diagnosed with autism but not have a learning disability.
The UK legislative framework dictates that parents with learning disabilities have a right to have children and to be supported in bringing them up (Human rights act 1998, Equality Act 2010 and Mental Capacity Act 2005). It is recognised that such parents may face a particular set of problems and challenges, including accessing antenatal care, understanding information about their pregnancy and birth choices or medical information about their baby. Parents may also be anxious about asking for or accepting professional help as they may believe that this will result in their child being removed from their care. Malouf et al (2016) concluded: ‘Mothers who will be subject to a social care assessment of their parenting skills need clear information about the process, their choices, and the level of skill they must demonstrate, as well as access to sufficient antenatal and postnatal support…’ If the parents/carers of the unborn child are already accessing support via adult services, the lead worker must be involved in any pre-birth assessment. If adult services are not involved, a referral to North Yorkshire or City of York Health and Adult Services should be explored with consent of the parents/carers and, with consent, a referral could be made for additional support to the Learning Disability Service, Disability Action Yorkshire. For more information on Good Practice guidance on working with parents with a learning disability, please see Children of Parents with Learning Disabilities.
‘Reasonable adjustments’ should be considered to support the parent(s) including the option of easy read information, extended or adapted appointments and having a hospital passport. People with learning disabilities and difficulties can also be supported by community-based services such as the Learning Disability Service.
- Neurodivergence in parenting – Neurodiversity refers to the natural variation in human brain function and behaviour and includes the full range of how brain functioning affects each person’s behaviour. Neurodivergence refers to individuals whose brains function in a way that is different from what is considered typical. Parents with neurodivergence, may experience significant emotional and psychological difficulties. Each type of neurodivergent condition presents its own specific challenges and strengths that can influence parenting. Neurodivergent parents often face societal assumptions and stigma that cloud perceptions of their parenting abilities. It is important for professionals have a good understanding of the impact of neurodivergence to ensure that their assessments are accurate. Neurodivergence in parenting – Ready to Relate
- Parents with significant physical health problems or disabilities which may make it difficult for them to care for a young child – There are around 1.7 million disabled parents in the UK, mostly with physical and sensory impairments. A report on a UK study on physically disabled parents’ experiences of maternity services reveals that physically disabled people embarking on parenthood face a number of challenges in getting appropriate information and support, including negative attitudes from some health professionals, a lack of knowledge and information available for parents and professionals, as well as poor communication between disabled parents and professionals.
- Young and/or unsupported parents – ‘Like all parents, young mothers and fathers want to do the best for their children. Whilst a good proportion of young parents manage very well, many young parents’ health, education and economic outcomes remain disproportionately poor, affecting the life chances for both them and their children. While every young parent has their own individual story, the risk factors for early pregnancy highlight the vulnerabilities with which some enter parenthood, including family poverty, persistent school absence, slower than expected school attainment and being looked after or a care leaver’ (Public Health England, 2019). This same report concluded that poor outcomes for the children of young parents can be mitigated by early coordinated and sustained support. (For tips working with fathers please see the North Yorkshire Safeguarding Children Partnership Working with Men Conference video).
- Parents who are Looked After or Care Leavers – Care‑experienced young people who become pregnant may benefit from early access to information, guidance, and support to help them make informed choices about their future. Where appropriate, they should be offered the opportunity to engage with relevant health professionals and, where available, specialist teenage pregnancy or young parent services.
We know that care‑experienced parents can thrive with the right support at the right time, and each young parent should be understood as an individual, not through assumptions based on the experiences of others. Professionals should work collaboratively and sensitively, recognising the potential for positive outcomes and ensuring support is tailored to the young person’s needs, wishes, and circumstances.
For young people who are looked after by the local authority, the allocated Social Worker has responsibility for coordinating access to services and for ensuring the Care Plan is kept up to date. This includes reflecting the needs and progress of each young parent in a way that is balanced, non‑judgemental, and focused on their strengths, safety, and wellbeing.
- Asylum seekers and families where English is not a first language – There is a five-fold difference in maternal mortality rates amongst women from Black ethnic backgrounds and an almost two-fold difference amongst women from Asian ethnic backgrounds compared to white women (Knight et al, 2018). There are also significant adverse pregnancy outcomes for their babies. Where English is not the first language, it is important to offer professional interpreter services and not to rely on family members to translate. The key issues for migrant, refugee and asylum-seeking women recently arriving in the UK include poor overall health status, language difficulties (as many do not speak English), and possibly chronic or unrecognised medical conditions such as malnutrition, HIV, hepatitis or tuberculosis.
The 2025 Child Safeguarding National Review Panel report highlights the importance of practitioners having conversations with families, children and young people about their race and identity in order to understand this in the context of their experience of being parented/parenting. Safeguarding partnerships should create conditions that empower practitioners to have conversations with children and families about race and identity, building skill and confidence. This includes ensuring there are safe opportunities for self-reflection within teams and in supervision to enable them to acknowledge their own biases. Key learning and recommendations centred on promoting opportunities for professionals to consider and promote all aspects of a child’s identity. Race, racism and safeguarding children – GOV.UK.
- Families who are homeless – Women who are pregnant and homeless constitute a unique group at significant risk of adverse foetal and maternal outcomes. Women can become homeless due to family breakdown, debt, poor mental health, and substance misuse problems which add to their vulnerability and those of the unborn infant. Robust, collaborative working is needed by all who provide social and healthcare services to homeless pregnant women, to improve the health outcomes for these women and babies. The key medical issues for pregnant women and their families who are homeless include poor overall health status, malnutrition, risk of blood borne virus infection, other infectious diseases including tuberculosis and skin infections, and unrecognised medical conditions.
Parental behaviours which may pose a risk to the child:
Domestic abuse –
Domestic abuse is any incident or pattern of controlling, coercive, threatening, violent, or abusive behaviour between people aged 16 or over who are personally connected, including physical, sexual, psychological, emotional, or economic abuse. Abuse can be perpetrated by partners, ex-partners and family members, including children under the age of 18, adult children or siblings. It may include one or more of physical or sexual abuse; violent or threatening behaviour; controlling or coercive behaviour; economic abuse; psychological, emotional and other forms of abuse. This definition includes honour-based abuse and forced marriage, and is clear that victims are not confined to one gender or ethnic group.
- Pregnancy can be both a trigger and risk factor for domestic abuse (DH, 2016) with 30% of domestic abuse starting or intensifying in pregnancy. 1 in 3 women experience domestic abuse during pregnancy (NHS, 2023).
- Domestic abuse is associated with an increased risk of miscarriage, still birth and premature birth (NHS 2018). It can also be linked to mental health concerns and substance misuse (DH, 2010). Domestic abuse also directly affects the unborn baby: by 18 weeks gestation the unborn baby can hear and by 24-26 weeks gestation the unborn will be startled by very loud noises outside the womb which can cause a stress response in the baby. If a pregnant woman is stressed or scared over a significant period of time, which often occurs where there is domestic abuse, increased levels of the stress hormone, cortisol, will cross the placenta to the unborn baby. Exposure to high levels of maternal cortisol during pregnancy may negatively affect the baby’s brain and overall child developmental outcomes.
Current use of drugs or alcohol –
Substance use by mothers/fathers/ partners and/or anyone that is involved in a child’s life does not on its own automatically indicate that children are at risk of abuse or neglect. However, where substance misuse is causing physical, psychological, social, interpersonal, financial and or legal problems, the implications for children and families must be thoroughly assessed. Drug and alcohol use during pregnancy, dependent on frequency and severity, can adversely impact the developing foetus, particularly during the first twelve weeks of gestation. Risks include increased risk of miscarriage, likelihood of premature delivery, reduced birthweight and head circumference, and an increased risk of Sudden Unexpected Death in Infancy. The infant exposed to drug or alcohol use during pregnancy is at increased risk of long-term cognitive and developmental problems.
Parents and carers with drug or alcohol problems may turn to crime to fund their dependency. This may mean exposing their children to unsafe adults or involving them in criminal activity.
Parental and family mental illness –
Perinatal mental health (PMH) problems are those which occur during pregnancy or in the first year following the birth of a child. Perinatal mental illness affects up to 27% of new and expectant mums and covers a wide range of conditions including anxiety, depression, and postnatal psychotic disorders (NHS England, 2026). These are collectively called perinatal mental illnesses. Fathers are also affected, with between a quarter and half of fathers with a partner with a perinatal mental illness being depressed themselves (Goodman 2004). If left untreated, mental health issues can have significant and long-lasting effects on the woman, the child, and the wider family. Some women are at an increased risk of experiencing mental illness in the perinatal period, particularly those who have had a previous history of mental illness. Women who have experienced postpartum psychosis, severe depression in the past or have a diagnosis of bipolar disorder have around a 50% chance of becoming unwell in the perinatal period (Oates, M, 2001; Jones, 2019).
If mental health challenges are disclosed during a pregnancy or the postnatal period, the practitioner should actively seek to confirm any formal diagnosis via liaison with primary care and/or mental health services, and ensure all appropriate support is in place.
Most families, where there is perinatal mental illness, manage very well and they are able to give their children safe and loving care. However, without the right support, perinatal mental illness can have an adverse effect on the baby’s brain development and long-term outcomes for the child (Centre on the Developing Child at Harvard University, 2009). Interactions with caregivers are the most important element of a baby’s early experience and help build secure and stable attachments. The nature of this early attachment sets the template for future relationships and can predict a number of physical, social, emotional, and cognitive outcomes (Cuthbert et al, 2011).
In more serious cases, parental mental illness increases the risk that a baby could be abused or neglected. Babies are particularly at risk if:
- Parents experience psychotic beliefs about the baby.
- Parental perinatal mental illness results in conflict or isolation.
- Parental perinatal mental illness significantly impairs a parent’s ability to function (Manning and Gregoire, 2008).
Much of the negative impact that parental perinatal mental health could have on the family and baby’s lives can be prevented. The quality of parental interactions with babies and the development of secure and stable attachment relationships can be improved through effective interventions (Hogg 2013).
The North Yorkshire and York Perinatal Community Mental Health Team provide a community service to support women who are experiencing mental health difficulties during pregnancy or in the first year after they have had their baby. Please review the link to determine if a referral to this service would be appropriate for the women you are working with.
https://www.tewv.nhs.uk/services/north-yorkshire-and-york-perinatal-mental-health-service
Many parents with mental health problems are able to give their children safe and loving care, without their children being negatively affected in any way. But sometimes, parents with mental health problems need support from family members, friends, neighbours and/or professionals, to help them care for their children.
It is important to understand the impact of parental mental ill health on the ability to provide safety for children in the family.
Practitioners are advised to utilise the North Yorkshire and York PAMIC Tool guidance to support their assessments in terms of need and risk.
Maternal ambivalence –
The analysis of Serious Case Reviews (DfE, 2016) recognised that ‘maternal ambivalence towards her child (both during and after pregnancy) was highlighted in many reviews as a potential indicator of a child’s vulnerability. At its extreme, this may present with a concealed or denied pregnancy. Whilst such cases are rare, other presentations including delayed antenatal booking or uncertainty about keeping the pregnancy are far more common.’ The report concluded that such presentations offer professionals (particularly in primary care and maternity services) opportunities to explore parental concerns and feelings towards the pregnancy and the unborn infant.
Whilst maternal ambivalence in pregnancy may not be considered a risk factor on its own, it becomes relevant when ambivalence is intense, persistent, and unsupported, it coexists with mental‑health difficulties, or it occurs in the context of domestic abuse, trauma, or social isolation. Understanding ambivalence early can help professionals recognise when a woman may need additional emotional or practical support.
Practitioners should consider whether avoidant behaviour may be rooted in trauma, rather than assuming it reflects deliberate resistance. This understanding is essential to safeguarding both current and future children. This principle should remain central to safeguarding practice. Practitioners should be mindful of how parents’ past experiences, including trauma, discrimination and negative encounters with professionals, can shape their ability or willingness to engage (Child Safeguarding Practice Review Panel, 2026).
Denial or concealment of pregnancy –
The concealment and denial of pregnancy will present a significant challenge to professionals in safeguarding the welfare and wellbeing of the unborn infant and the mother. Lack of antenatal care in concealed or denied pregnancies can mean that potential risks to mother and child are not detected. The health and development of the baby during pregnancy and labour may not have been monitored or foetal abnormalities detected. It may also lead to inappropriate medical advice being given, such as potentially harmful medications prescribed by a medical practitioner unaware of the pregnancy. The potential risks to a child through the concealment of a pregnancy are difficult to predict and are wide-ranging.
While concealment and denial, by their very nature, limit the scope of professional help, better outcomes can be achieved by coordinating an effective multi-agency approach. Follow associated practice guidance:
Concealed, Denied or Late Presentation of Pregnancy
Surrogacy –
Surrogacy is an arrangement whereby a woman gets pregnant and gives birth on behalf of another person or couple who will become the child’s legal parents after birth. It is legal in the UK providing the surrogate receives no payment beyond what would be classed as reasonable expenses. Surrogacy through commercial means, however, is illegal in the UK and therefore it is an offence for an individual or agency to act on a profit-making basis to organise or facilitate surrogacy for another person.
When any professional is made aware of a pregnancy as a result of a surrogacy arrangement, they must make the necessary enquiries to satisfy themselves of the legitimacy of the arrangement i.e. that the treatment was undertaken by a licensed clinic. It is advised that written evidence is obtained to confirm this.
If professionals are satisfied the surrogacy is through a licensed clinic, the local authority does not need to be informed unless there are other concerns raised that indicate that the unborn baby may be a risk.
Where the circumstances of the conception and subsequent arrangements for the baby are unclear, professionals should contact their safeguarding children lead for further advice and a referral to Children and Family Services may be required to allow for further enquiries to be made.
Further information can be found:
Surrogacy Arrangements Act 1985
Current or previous history of safeguarding concerns:
- Where a previous child to both or either parent has been removed from their care due to safeguarding concerns.
- Previous unexpected death of a child whilst in the care of either parent or other adult in the household where abuse or neglect is/was suspected.
- A parent or other adult in the household is a person identified as presenting a risk, or potential risk, to children.
- Children in the household/family currently subject to a Child Protection Plan or previous child protection concerns.
- Where a previous child within the family, for either parent, is living outside of their care, practitioners need to establish why this is and if it relates to any previous safeguarding concerns.
- Parent previously suspected of fabricating or inducing illness in a child.
- Families where there is a history of Female Genital Mutilation (FGM), honour-based violence, forced marriage or suspected trafficking.
- Significant mental health concerns, particularly where a postnatal mental health issues, such as puerperal psychosis, have led to safeguarding concerns for previous children
- Where a parent/carer or significant family member is subject to MAPPA arrangements (Multi agency public protection arrangements) or MARAC (multi agency risk assessment conference) arrangements
Female Genital Mutilation (FGM) and Unborn Babies
Where Female Genital Mutilation is identified in pregnancy, an honest and open conversation should take place between the practitioner, pregnant woman and her partner. Professionals should seek support from their organisation’s translation services if required rather than rely on relatives or friends. The practitioner should share the opposing statement, which can be obtained in the women’s first language. Professionals should follow the City of York and North Yorkshire Safeguarding Children Partnership Practice guidance on Female Genital Mutilation.
Working with Fathers
- It is important that all agencies involved in pre and post birth assessment and support, fully consider the significant role of fathers and wider family members in the care of the baby even if the parents are not living together, and where possible, involve them in the assessment. This should include the father’s attitude towards the pregnancy, the mother and newborn child, and his thoughts, feelings and expectations about becoming a parent. It should also include the father’s history and previous experience of parenting.
- Information should also be gathered about fathers and partners who are not the biological father at the earliest opportunity to ensure any risk factors can be identified.
- A failure to do so may mean that practitioners are not able to accurately assess what mothers and other family members might be saying about the father’s role, the contribution which they may make to the care of the baby and support of the mother, or the risks which they might present to them. Background police and other checks should be made at an early stage on relevant cases to ascertain any potential risk factors.
- In the majority of cases where babies have been injured or killed, men are the perpetrators – research suggests that men are between 2 and 15 times more likely than women to cause this type of harm in under 1s. The greater prevalence of male abusers sits alongside a description of men as too often being ‘hidden’ or ‘invisible’ to safeguarding agencies. The Myth of Invisible Men (Child Safeguarding Practice Review Panel, 2021).
- Involving fathers in a positive way is important in ensuring a comprehensive assessment can be carried out and any possible risks fully considered. One of the consequences of the failure to routinely find, engage and assess men is that the protection of children to whom they present a risk often falls on mothers. Too often mothers are left to manage those risks on their own and are faced with the potential or real removal of their children, if they are seen to have failed to protect their children.
- Further information and resources in relation to fathers is available on the City of York Safeguarding Children Partnership website.
Referrals to Children’s Social Care
Practitioners should use this guidance and the local Threshold of Need guidance (click here to access North Yorkshire’s “Framework for Decision-Making: Right help, at the right time by the right person” or click here to access City of York Threshold Document) to determine if the parents may need support services to care for their baby or that the baby may have suffered, or be likely to suffer, significant harm. Often the presenting issues do not warrant a safeguarding referral to CSC/ CFS and that the offer of early help is the most appropriate way forward. In these circumstances, gain consent from the parent (s) and follow the local pathways for early help interventions.
- Referrals to Children’s Social Care should be made from 12 weeks gestation and no later than 16 weeks, by any practitioner working with the family. It may be that concerns are not known until later in the pregnancy at which point a referral should be made as soon as concerns are identified. There are times when it may be necessary to consider a referral before 12 weeks. In these situations, practitioners should discuss circumstances and rationale with the safeguarding lead within their organisation prior to referral and not await midwife confirmation of pregnancy.
- Referral at this early stage in the pregnancy will:
- Provide sufficient time for a full and informed assessment.
- Provide sufficient time to make adequate plans for the baby’s protection.
- Avoid initial approaches to parents in the last stages of pregnancy, at what is already an emotionally charged time.
- Enable parents to have more time to contribute their own ideas and solutions to concerns and increase the likelihood of a positive outcome for the baby.
- Enable the early provision of support services so as to facilitate optimum home circumstances prior to the birth.
- On receipt of the referral, Children’s Social Care will make a decision as to how to proceed, within one working day.
It is important to note that Statutory Guidance for Court Orders and Pre-Proceedings for Local Authorities states that:
“Where the local authority is considering proceedings shortly after birth, the timing of the sending of the pre-proceedings letter or letter of issue should take account of the risk of early birth and help to ensure that discussions and assessments are not rushed. Ideally the letter should be sent at or before 24 weeks” (p 19).
It is best practice to complete and share the pre-birth assessment at least 4 weeks prior to birth to afford appropriate time for families to consider this.
The City of York pre-birth panel is based on the ‘Born into Care’ best practice guidance and brings multi-agency partners together with social care practitioners to support and strengthen practice related to unborn babies and their families. The panel reviews all referrals for unborn babies to help ensure that needs are identified and that the right people are involved. The Panel also adopts and tracks cases which look likely to benefit from additional oversight and support due to identified risks and/ or complexity.
- Although most referrals will not require legal proceedings, it is important to bear in mind the timescales laid out in the guidance as they will not be met unless referrals are made at an early stage in the pregnancy.
It should also be noted that overall, around 7% of babies are born early and that maternal substance use, a major issue for child protection, is associated with premature birth.
Where appropriate, early pre-proceedings meetings provide more opportunity for advice and discussion to influence the parent, and for the parent to influence the local authority’s plans. Parents-to-be have more time to demonstrate that they can work with professionals in preparing for the baby, and professionals have more time to assess them and any carers they propose. Pre proceedings meetings should take place before 26 weeks wherever possible.
Consent
Concerns should be shared with both prospective parent/s and it is good practice to gain consent to refer to the relevant Local Authority Children’s Social Care. Every effort should be made to be open and honest about concerns and work in partnership with parents at this early stage ensuring they are aware of what the professional concerns are and how a referral to Children’s Social Care will support them. However, if obtaining consent may place the welfare of the unborn child at risk, this should be avoided e.g., if there are concerns that the parent/s may move to avoid contact with investigative agencies. Where a referral is made without consent, the rationale for making the referral should be documented and recorded.
Pre-Birth Assessments
A pre-birthassessment should be offered on all pre-birth referrals that reach the threshold for Children’s Social Care. The assessment should be commenced as early as possible, preferably before 16 weeks. All partner agencies who are involved with either the parents, unborn baby or siblings have a duty to contribute towards the pre-birth assessment.
In the following circumstances a Strategy Meeting must be convened:
- A parent or other adult in the household, or regular visitor, has been identified as posing a risk to children.
- A sibling in the household is the subject of a Child Protection Plan. If the unborn baby has siblings on Child Protection Plans, an Initial Child Protection Conference on the unborn baby must be convened. This could, if appropriate, be incorporated into a Review Child Protection Conference for the older siblings.
- A sibling has previously been removed from the household either temporarily or by court order.
- There is evidence of domestic abuse in the unborn baby’s household.
- The degree of parental substance use is likely to impact significantly on the baby’s safety or development.
- The degree of parental mental illness/impairment is likely to impact significantly on the baby’s safety or development (see PAMIC tool). This includes where there are acute professional concerns regarding parenting capacity, particularly where the parents have either severe mental health problems or learning disabilities.
- There are significant concerns about parental ability to self-care and / or to care for/protect the child e.g. unsupported, young or learning-disabled mother. This includes where the expectant mother is not engaging in ante-natal care.
- Any other concern exists that the baby may have suffered, or is likely to suffer, significant harm, including a parent previously suspected of fabricating or inducing illness in a child or harming a child.
- A child aged under 13 is found to be pregnant (due to classification as statutory rape – Sexual Offences Act, 2003)
- Where the expected parent is very young and a dual assessment of their own needs, as well as their ability to meet the baby’s needs, is required. (If the expectant mother is a child/young person, or an open case to Children’s Social Care they must have an allocated Social Worker in their own right).
Birth Response Plan
All unborn babies subject to a Child Protection Plan must have a written Multi-Agency Birth Response Plan (BRP) before the women is 34 weeks pregnant. This plan should be agreed at either the child protection conference or within the Core Group.
The Birth Response Plan must include the following elements:
- Planned duration of hospital stay.
- Whom to notify when baby is born, including EDT (Emergency Duty Team).
- Contact arrangements for parents, extended family members and significant others.
- If supervision is required, who is the agreed supervisor?
- Details of any pending legal processes.
- What to do if the Birth Response Plan is not followed.
The Birth Response Plan should be formed with parents unless to do so is felt to put the mother or baby at increased risk of harm. Professionals will need to agree how the plan will be shared with parents and who will lead this conversation.
Copies of the Birth Response Plan should be held by all agencies responsible for taking forward the child protection plan including, the midwifery unit where it is agreed the baby will be delivered, the community midwife, the allocated Social Worker and the Children’s Social Care Emergency Duty Team.
Pre-Discharge Planning Meetings
The discharge planning process should be initiated as soon as the mother is admitted/presents for delivery and all midwives caring for her should have full access to and knowledge of the BRP. Following the birth and prior to discharge from the maternity unit, a Pre-Discharge Planning Meeting must be held. This meeting should be convened by the Social Worker in conjunction with the maternity staff.
The newborn baby should not be discharged at weekends or on bank holidays unless there is a consensus of opinion that it is safe and reasonable to do so. This is documented in the child’s medical record and discharge plan.
Who should be present:
- Parents (if appropriate).
- Community Midwife.
- Postnatal Ward Staff.
- Social Worker.
- Foster Carer (where appropriate).
- Wider family (where appropriate).
- A member of the Trust Safeguarding Team.
- Health Visitor.
- Other agencies which may need to be involved should be considered, dependent on the circumstances, such as police, mental health colleagues, learning disability colleagues, GP, the local authority legal team and any other key professionals that are in a position to support the safeguarding of the newborn.
Multi-agency Discharge Plan
An agreed multi-agency discharge plan will set out arrangements for the care and safety of the child following discharge from hospital into the community and will include actions, timescales and responsibility for actions. The agenda for the discharge planning meeting is as follows:
Discharge Planning Meeting Agenda
- Introductions and purpose of meeting
- Professionals attending and apologies
- Clarify name, date of birth, address, ethnicity of the child and significant family members, including other children
- Agency updates in relation to pre-birth and post birth considerations during hospital stay
- Discharge plans will include:
- When and to whom the baby is to be discharged.
- Reasons why this is the proposed plan.
- Views of the parents on the proposed plan.
- Is parental consent required to implement this plan? If not, detail how consent will be dispensed with.
- Consideration of the baby’s development and whether or not there are specific medical needs which need to be addressed, including how these will be addressed.
- How and when a pre-birth visit will be undertaken, who will undertake this and also include discussion about home safety and safe sleeping.
- Who will transfer/ transport the baby and/or parent/s to the proposed address?
- What equipment is required and who will provide this e.g., car seat, clothing, feeding equipment.
- Consider any equality and diversity issues in relation to the baby and the family and how these may impact on implementation of the plan.
- Contingency plans.
6. Consideration of support needs for other siblings, parent/s and significant family members, including how and who will provide this.
7. Where there is a plan to separate the baby from their parents – how will the baby maintain their relationship with their parents and family, consideration about expressed breast milk if mother is breast feeding, and how will this be supported.
8. Consider information to be shared or withheld from parent/s and the reasons for this.
9. Arrangements to inform (including who and when)
- The Community Midwife.
- The Health Visitor.
- General Practitioner.
- Where appropriate, any other agencies involved such as: police, mental health colleagues, learning disability colleagues, local authority legal team and any other key professionals that are in a position to support the safeguarding of the newborn.
10. Proposed multi-agency visiting arrangements following discharge.
11. Dates for review of arrangements.
References
Department of Health (2001) Valuing People: A New Strategy for Learning Disability for the 21st Century. London: The Stationery Office. Available at: https://www.gov.uk/government/publications/valuing-people-a-new-strategy-for-learning-disability-for-the-21st-century
Center on the Developing Child at Harvard University (2009) Maternal Depression Can Undermine the Development of Young Children: Working Paper No. 8. Cambridge, MA: Harvard University. Available at: https://developingchild.harvard.edu/resources/working-paper/maternal-depression-can-undermine-the-development-of-young-children/
Child Safeguarding Practice Review Panel (2026) Protecting all vulnerable babies better: National review into the broader safeguarding issues raised by the death of baby Victoria Marten.
Child Safeguarding Practice Review Panel (2021) The Myth of Invisible Men.
Confidential enquiry into maternal and child health for England and Wales (2001) Why mothers die 1997-1999. London: RCOG Press.
Cuthbert, C, Rayns, G & Stanley, K (2011) All Babies Count: Prevention and protection for vulnerable babies. NSPCC:London
Department for Education (2016) ‘Pathways to Harm, pathways to protection: a triennial analysis of serious case reviews 2011 – 2014’ Accessible at: https://www.gov.uk/search/all
Department for Education (2022) ‘Learning for the future: final analysis of serious case reviews, 2017 to 2019’ Accessible at Learning for the future: final analysis of serious case reviews, 2017 to 2019
Department of Health and Social Care (2018) ‘Care in Surrogacy: Guidance for the care of surrogates and intended parents in surrogate births in England and Wales’ Accessible at https://www.gov.uk/government/publications/having-a-child-through-surrogacy
Department of Health (2016) ‘Responding to domestic abuse: A resource for health professionals’ https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/597435/DometicAbuseGuidance.pdf
Department of Health (2010) ‘Responding to violence against women and girls –the role of the NHS: The report of the Taskforce on the Health Aspects of Violence Against Women and Children’ Accessible at: https://www.bestbeginnings.org.uk/Handlers/Download.ashx?IDMF=9d83788e-748e-416f-9069-e142e86e3ebe>
Goodman, J (2004) Paternal postpartum depression: it’s relationship to maternal postpartum depression and the implications for family health; Journal of Advanced Nursing 45(1) pp26-35
Hogg, S (2013) Prevention in Mind: All Babies Count: Spotlight on Perinatal Mental Health. NSPCC:London
Jones, I (2019) Bipolar disorder, Pregnancy and Childbirth. Bi-polar UK & Action Postpartum psychosis: https://www.app-network.org/wp-content/uploads/2012/03/bipolar_uk_bipolar_disorder_pregnancy_childbirth.pdf (Accessed 28/03/19)
Knight M. et al (2018) ‘Saving Lives, Improving Mothers’ Care: lessons learnt to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2014–16’ MBRRACE-UK, University of Oxford.
Malouf R et al (2017) ‘ “We just wanted to be normal parents”: a qualitative study of the experience of maternity care for women with a learning disability’ BMJ Open 2017;7:e015526. doi:10.1136/bmjopen-2016-015526
Manning, C, Gregoire, A (2008) Effects of Parental illness on Children; Psychiatry 8(1)
National Health Service (2018) ‘Domestic Abuse in Pregnancy’ Accessible at: <https://www.nhs.uk/conditions/pregnancy-and-baby/domestic-abuse-pregnant/>
National Health service (2026) Perinatal Mental Health
National Health Service (2023) Getting help for domestic violence and abuse – NHS (accessed 13/03/26)
NHS England (2026) NHS England » Perinatal mental health (accessed 23/03/26)
Oates, M (2001) Perinatal maternal mental health services: Recommendations for provision of services for childbearing women. Royal College of Psychiatrists: London
O’Hara, M, Swain, A (1996) Rates and risk of postpartum depression-a meta-analysis; Int Rev Psychiatry 8 pp37-54
Public Health England (2019) A framework for supporting teenage mothers and young fathers. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/796582/PHE_Young_Parents_Support_Framework_April2019.pdf (Accessed 05.08.19)
Taft, A (2002) ‘Violence against women in pregnancy and after childbirth’ Current knowledge and issues in healthcare responses Australian Domestic and Family Violence Clearinghouse: Issues Paper 6.
Page reviewed: July 2026

 View all our news
View all our news